

The “Brain Efficciency Training’’ Mentamove® is a neuro-rehabilitation method is used for the rehabilitation after various brain lesions. If the motoric activities are mentally practised by the subject with Mentamove®, the real movement gives a reorginasation to the brain due to neuroplastisity.
EMG-initiated muscular stimulation (EMG Guided Therapy) gives is aneffect mainly used in the treatment of stroke patients.
It is a combination of muscular stimulation with medium frequency sine current and a biofeedback proces. It can be used after ischemic stroke, hemorrhagic stroke, trauma or inflammation of the CNS(Fig. 1) (1).
Methods
Our case has a cloth (2.5×2.5 cm) at left thalamus (CapsulaInterna) after head injury(Fig. 2). He (27 years old, male) had right hemiplegia (Fig 6,7) with mild central type fascial paralysis(Fig 8) and aphonia(voice redicing) after a traffic accident. After cloth resorbtion(Fig.3,4)the method used on the right shoulder (m. supraspinatus and m. deltoideus), elbow (m. triceps brachii), wrist (m.extensor digitorum, m. extansor carpi ulnaris, m.extansor carpi radialis longus and brevis), hip (m. quadriceps femoris), knee and peroneal (m. tibialis anterior) muscles 2 times/daily device during 2 months. Every seasons duration was 20 minutes. Outcome monitorised by the Medical Research Council Scale (MRC) of 0-5 (Table 1), and video documentation and photografic documentation and brain activity investigated during finger taping bilaterally and right foot dorsiflexion movements with fMRI (GE Signa 1.5 TESLA MRI) before (Fig 5) training and after 2 months of the treatment. The movements activity took 30 sec.and rest period took 30 sec. during 8 minutes of the investigation with fMRI.




Outcome and Activity
The subject not supported with any extra rehabilitation method. After 5 days he begun to walk. After 15 days he showed sitting alone, and begun to walk without ascistence (Fig 6).
After 1 month he showed right arm abduction activity from shoulder, and little elbow extantion, but no finger activity on the right hand (Fig 6,7). The right leg shows hip flexion and knee extention, and he can stand alone on the right leg without any support. The foot dorsiflexion none. (Fig 6,7).
After 2 months of the therapy he showed right arm abduction overhead againts to the gravity (Fig 8) and motor power on the right leg to the against to pressing (Fig 9).
After 2 months the case stopped working, because he found it enough to do dailiy activities alone. After 3 months of the therapy he investigated with fMRI. The daily activities increased spontaneusly, he begun to work after 6 months of the therapy.

Results: The motor power of the shoulder abduction, elbow extension, hip flexion and knee extension increased from 0 to 5 point, and wrist extansion, dorsiflexion 0 to 4+, point due to MRC scale (Table 1). The neurologic condition before treatment demonstrated at the Fig 6, 7, 8. 9. The outcome and daily activity demonstrated at the Fig 6, 7 after 15 days, at the Fig 7 after 1 month, and the Fig 8, 9 after 2 and 3 months of the therapy.
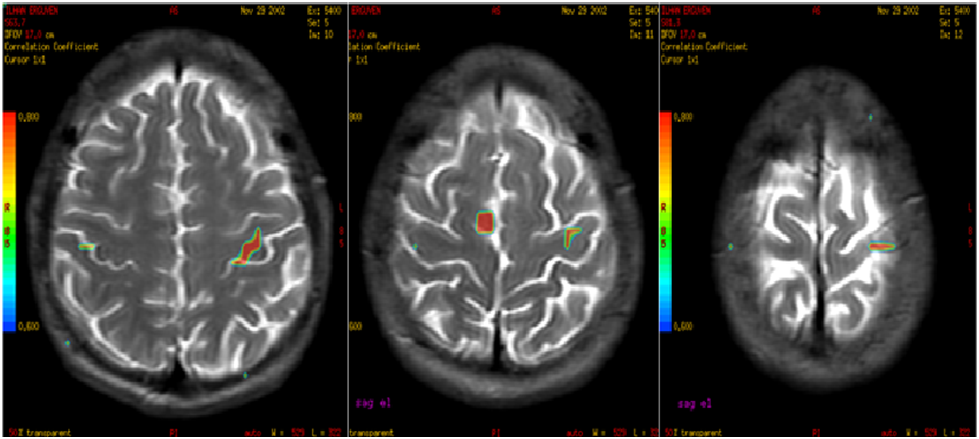
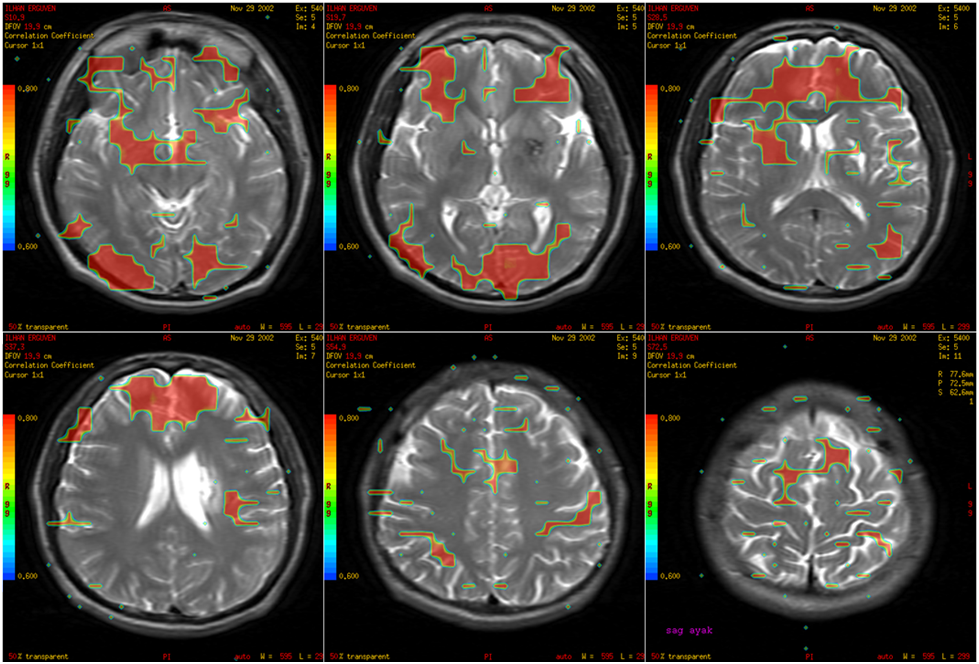
The fMRI investigation after 2 months of the therapy well done. The fMRI showed BOLD (Blood Oxygen Level Dependence) activity on both motor cortices before treatment (Fig 5). After 2 months fMRI showed increased BOLD activity on the right premotor cortex with right hand movements as difference from left hand finger taping (Fig 21). The left hand finger tapings showed no difference from normally anatomic localisation (Fig 23,24,25). The fMRI showed an increased activity on the orbitofrontal cortex and frontal cortex bilaterally, left hipocampus, right thalamus, both premotor cortices with right foot dorsiflexion (Fig 10, 11, 12). The right side basal nuclei BOLD activity was more than the right thalamic activity.

Conclusion
Our case worked about 75 days with mentamove® method. And his neurologic deficits showed a recovery step by step in a short period. The muscle tonus was increased without any spasticity. The deep tendone reflexes were normally after 15 days without any asimetry. The fascial assimetry recovered spontanusly, the aphonia recovered after 2 months. In the first week of the therapy he showed a pulmonary tromboembolism due to stimulating of the peroneal muscles. He was threat with Heparine 10.000 IU/Day. The mentamove therapy stopped for 10 days. Clinically our results show an early mobilisation without any assistance and walker. The mentamove® application gave up a motoric support to the leg for walking. We wondered the brain motor cortical activity before of the treatment with mentamove®. So we investigated it with fMRI. The fMRI showed a bilateral motor cortical activity on each motor cortices (Fig 5). It was not surprised us because the lesion was on the white matter (on the left corticospinal tractus). The left motor cortex activity explains the finger taping tasks mentally. But we cannot see movement on the right hand.
The mentamove® therapy bases on the learning process of the idemortoric training, then the brain reorganises itself again (2,3,4). The brain memorial activities measured by Thomas Kammer at all (1997) with fMRI (5). They showed the orbitofrontal cortex and prefrontal cortex activity on the normal subjects during working memory. The prefrontal corex, orbitofrontal cortex, hippocampus and other liymbic system structures are very important for relearning and learning procedures. Our subject worked about 75 days for different places on the right extremities. But we programmed the application of courses due to the motor cortex anatomic organisation. The treatment everyday begun from peroneal muscles, hip muscles, shoulder, elbow and wrist muscles. Every course gives him a positive effect with muscular stimulation and physiologically brain accepts the proprioseptive activities by spinothalamic tractus. When the subject works with mentamove® he recalls his movements, then he has concentrated himself for every positive activity. He thinks how can increase his wrist extension. This aim increases the memory working as concentration and to be carefull. The fMRI with finger taping showed an increased activity on the right premotor cortex and it explains the subjects thought the movement during activity (Fig 10). Our fMRI data showed increased activity on the bilateral orbitofrontal and frontal cortex with foot dorsiflexion (Fig 10,11,12). And also the left hippocampal BOLD activity increased (Fig 26). The hippocampus is a center of the long term memory. The different data of the fMRI (increased BOLD activity) is showed on the right basal nuclei. There is high level BOLD activity from left side nuclei. This may be explained by right premotor cortex – corticospinal tractus trajectory and right basal nuclei activation.
All these data of fMRI may explain a new reorginasation of the brain after the Mentamove® rehabilitation method, after clinically recovered of hemiplegia due to capsula interna injury.
Abstract ID: A 0154
The Mentamove Rehabilitation After Head Injury Patient with Left Thalamic Hematoma: Case Report
Z. Akgun1, M. Akgun2, C. Garner3
1 Uludag University School of Health PhD, TURKEY, 2 State Hospital of Bursa MD Neurosurgery, TURKEY, 3 KWA Clinic Stift Rottal Neurology and Neurorehabilitation MD, GERMANY
Background: The “Brain Efficiency Training’’ Mentamove® is a neuro-rehabilitation method is used for the rehabilitation after various brain lesions. If the motoric activities are mentally practised by the subject with Mentamove®, the real movement gives a reorginasation to the brain due to neuroplastisity.
Methods: Our case has an cloth (2.5×2.5 cm) left thalamus after head injury. He (27 years old, male) had right hemiplegia with mild central type fascial paralysia and aphonia. After cloth resorbtion the method used on the right shoulder, elbow, wrist, hip, knee and peroneal muscles 2 times/daily device during 2 months. Outcome monitorised by the Medical Research Council Scale (MRC) of 0-5, and brain activity investigated with fMRI before training and after 2 months of the treatment.
Results: The motor power of the shoulder abduction, elbow extension, hip flexion and knee extension increased from 0 to 5 point, and wrist extansion, dorsiflexion 0 to 4+, point due to MRC scale.
The fMRI showed BOLD (Blood Oxygen Level Dependence) activity on both motor cortices before treatment. After 2 months fMRI showed increased BOLD activity on the right premotor cortex with right hand movements. Increased activity on the orbitofrontal cortex bilaterally, left hipocampus, right thalamus, both premotor cortices with right foot dorsiflexion. The left side basal ganglia activity was lower than the right thalamic activity.
Conclusion: These results of fMRI show new reorginasation of the brain after the Mentamove® rehabilitation method.
References
- R. Crisan, C. Garner:Effectiveness of EMG-initiated muscular stimulationin outpatients one year post-strokeNeurologie &Rehabilitation 6/2001, HippocampusVerlag, ISSN 0947-2177, S. 228-232.
- Adams JA (1971): A closed-loop theory of motor learning. J. Motor Behav 3, 111-49
- Alfieri V (1982): Electrical treatment of spasticity. Reflex tonic activity in hemiplegiepati-ents and selected specific electrostimulation. Scand J. Rehabil Med 14, 177-82
- Bach-y-Rita P (1981): Brain plasticity as a basis of the development of rehabilitation pro-cedures for hemiplegia. Scand J Rehab Med 13, 73-83
- T. Kammer, M.E. Bellemann, F. Gückel, G. Brix, A. Gass, H. Schlemmer, M. Spitzer: Functional MR Imaging of the Prefrontal Cortex: Specific Activation in Working Memory Task; Magnetic Resonance Imaging, Vol 15, No:8, pp:879-889, 1997, Elsevier Science Incl. 1997.
Kaynaklar ve Benzer Vakalar
- https://drmustafaakgun.com/mentamove-ile-rehabilitasyon/
- https://drmustafaakgun.com/the-mentamove-rehabilitation-2/
- https://drmustafaakgun.com/akut-spinal-kord-kompresyonu-sonrasi-paraplejide-mentamove-tedavisinin-etkisi-olgu-sunumu/
- https://drmustafaakgun.com/paraparezi-ve-mentamove/
- https://drmustafaakgun.com/bilateral-distal-paraplejide-mentamove/
- https://drmustafaakgun.com/kafa-travmasi-sonrasi-mentamove/
- https://drmustafaakgun.com/beyin-etkin-calisma-egitimi/
- https://drmustafaakgun.com/mentamove-metodu-ile-rsd-refleks-sempatik-distrofinin-tedavisi/
- https://drmustafaakgun.com/foot-drop-mentamove-metodu/
- https://drmustafaakgun.com/the-mentamove-rehabilitation/
- https://drmustafaakgun.com/the-oculomotor-palsy-after-right-posterior-communicant-aneurysm-surgery-and-treatment-with-mentamove-case-report/
- https://drmustafaakgun.com/mentamove-rehabilitasyon-nedir/
- https://drmustafaakgun.com/category/norolojik-rehabilitasyon/
- https://drmustafaakgun.com/mentamove-tedavisi/


