Beyin Etkin Çalışma Eğitimi (Mentamove®), çeşitli beyin lezyonlarından sonra rehabilitasyon için kullanılan bir nörorehabilitasyon yöntemidir.
M. Akgun1, B. Hakyemez2, Z. Akgun3, C. Garner4
1 State Hospital of Bursa Neurosurgery MD, TURKEY, 2 State Hospital of Bursa Radiology MD, TURKEY, 3 Uludag University School of Health PhD, TURKEY, 4 KWA Stift Rottal Clinic Neurology and Neurorehabilitation MD, GERMANY
Keywords: Cerebrovascular Disorders, Stroke. Hemiparesis, Spasticity, Electromyography, Rehabilitation, Biofeedback, Electrotherapy, Brain Efficiency Training, Mentamove®, Relearning, fMRI, Neuroplasticity, Brain Plasticity
اضطرابات الأوعية الدموية الدماغية ، السكتة الدماغية. الشلل النصفي ، التشنج ، تخطيط كهربية العضل ، إعادة التأهيل ، الارتجاع البيولوجي ، العلاج الكهربائي ، تدريب كفاءة الدماغ ، Mentamove® ، إعادة التعلم ، الرنين المغناطيسي الوظيفي ، المرونة العصبية ، لدونة الدماغ
Background: Brain Efficiency Training (Mentamove®) is a neurorehabilitation method used for rehabilitation after various brain lesions. If the motoric activities are mentally practiced by the patient, the real movement gives a reorganisation effect to the brain.
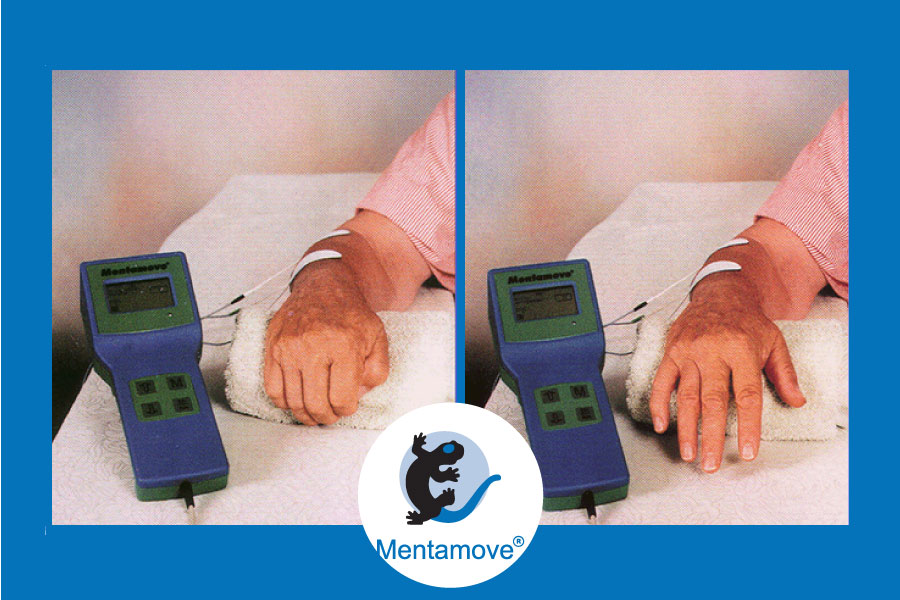
EMG-initiated muscular stimulation gives is an effect mainly used in the treatment of stroke patients. It is a combination of muscular stimulation with medium frequency sine current and a biofeedback process (Fig 1.2)
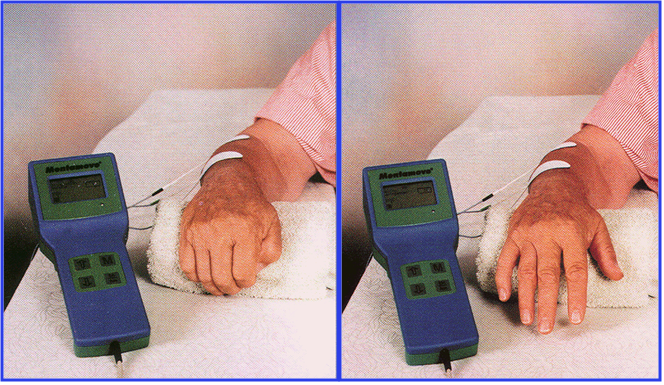
Fig. 1: The picture on the left shows the contraction phase when the patient mentally carries out a movement. As soon as the EMG exceeds the threshold pre-set by Mentamove®, muscular stimulation is triggered as shown in the picture on the right. Thinking to open fingers increases the EMG signals on the muscles, then EMG amplitudes increase from the base level, then electrostimulation did. After electrostimulation, the real contraction of the extensor muscles of the wrist opens the fingers and does wrist extension. Movements of the fingers and wrist give a positive effect on the Central Nervous System in afferent ways.

Fig. 2: EMG controlled back coupling is a real time working system for paretic subjects
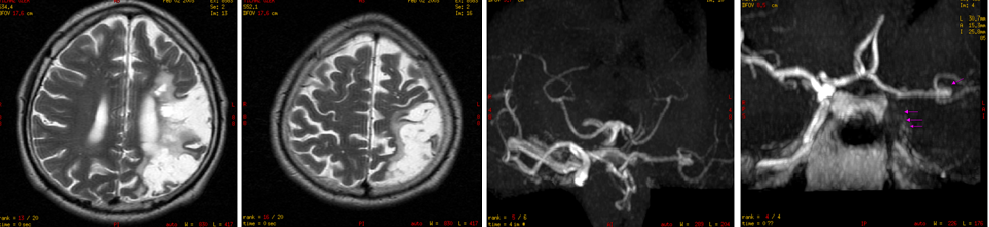
Method: Our case (53 years old, left-handed male) had left carotid artery occlusion. He still displayed right-side spastic hemiparesis (Ashworth 4 point) 15 months after the stroke, with motor dysphasia, and cognitive, memorial, and recalling problems (Fig 3).
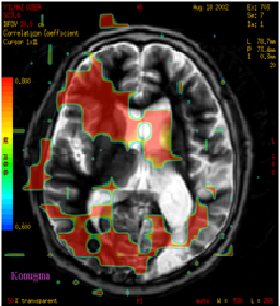
The control cranial MRI showed left parietal, occipital and temporal ischemic area due to the left middle cerebral artery occlusion, and MRI angiography showed left Carotid Artery Ocllusion after 28 months of stroke. And incidental aneurysm was seen on the left MCA bifurcation (Fig 4).
The Mentamove® training program was applied only on the right shoulder, arm, and forearm. The m. Supraspinatus and m. Deltoideus and trained 1 time/daily for shoulder abduction. M. Triceps Brachii trained 1 time/daily for elbow extension. M.Extensor Digitorum, m. Extansor Carpi Ulnaris, m.Extensor Carpi Radialis Longus and Brevis trained for wrist extension 1 time/daily. Every season’s duration was 20 minutes. The case worked for 5 months (Fig 5).
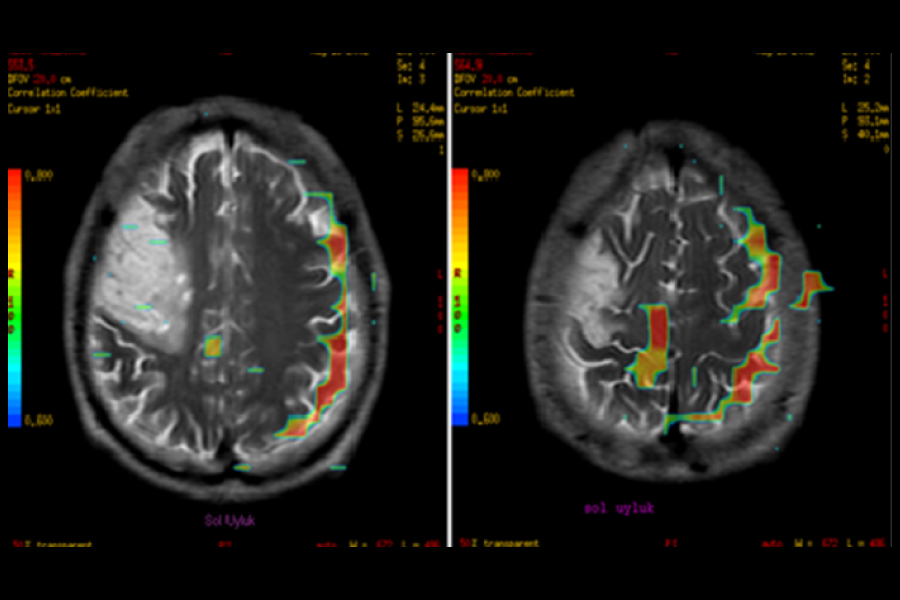
The results were measured with the Medical Research Council Scale (MRC) of 0-5 and video documentation and photographic documentation. The resulting brain activity was investigated with fMRI after 3 months, and 8 months after the use of the Mentamove® treatment. We investigated the left-hand movements (for comparative control with finger taping), right-hand movements (finger taping) and talking (repeat a word), tongue movements, and right-hand sensorial activity with 1.5 TESLA GE MRI. The movement activity took 30 sec. and the rest period took 30 sec. During 8 minutes. (Fig 23,24,25,26,27,28,29,30,31,32,33,34,35).


Results
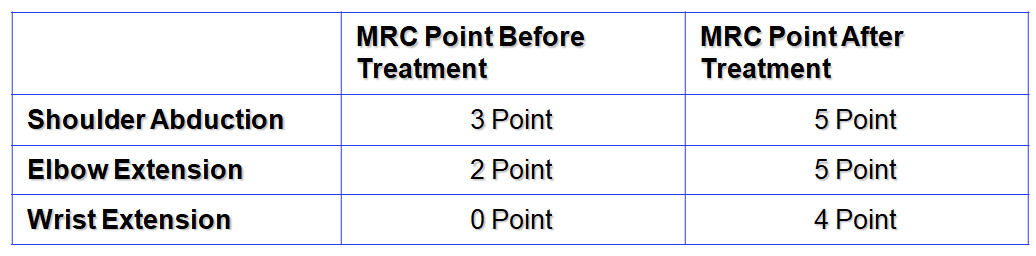
Using the MRC scale, the motor power increased on the right shoulder abduction from 3 to 5, and the elbow extension improved from 2 to 5. The wrist extension improved from 0 to 4 (Table 1). The therapy duration was 5 months.
Clinically the spasticity reduced from 4 to 1 point due to Ashworth on the right arm after 3 weeks. He began to catch glass after 15 days (Fig 6), and grasp a bottle, after 25 days (Fig 7), then he began to use a pencil carefully (Fig 8,9). The cognitive and memory functions (recalling, concentration, reading, finding an address, use of telephone and bank credit card) step by step increased after 35 days. The motor dysphasia was reduced step by step in 3.5 months. After 5 months of therapy, he has begun to talk in front of audiences at our conference (Fig 10). Interestingly he showed an activity like a right-handed man, spontaneously after 3.5 months (Fig 11). After his right arm movements were better than before therapy (Fig 12, 13, 14, 15).
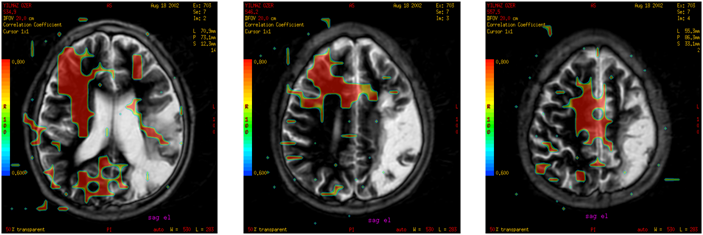
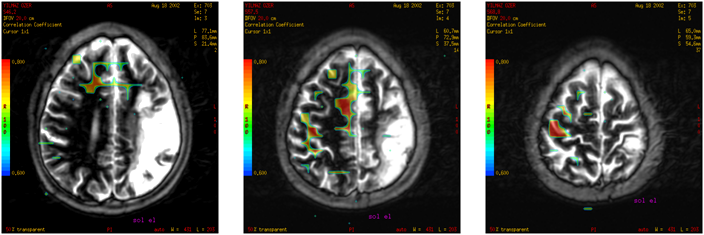
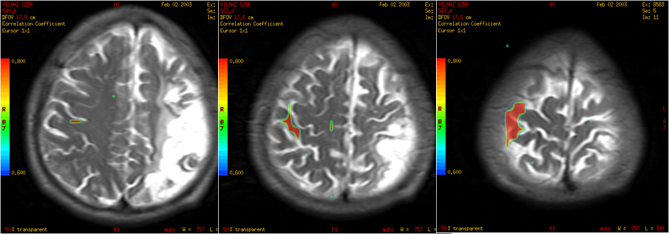
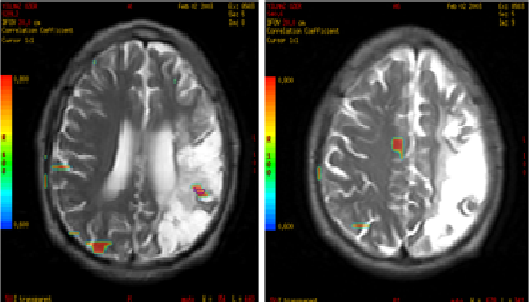
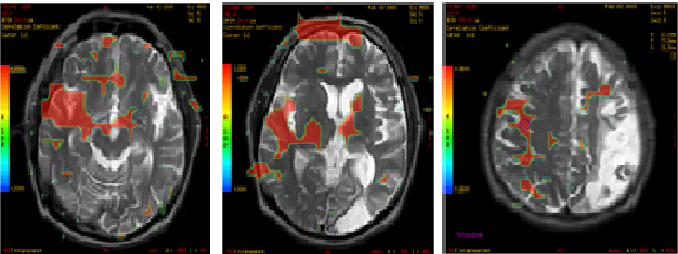
We investigated the brain motor cortex activity with 1.5 Tesla MRI (GE Signa) during left and right-hand finger taping and talking with repeating a word after 2 months of the therapy. Right-Hand Finger Taping. showed (Increased BOLD activity on the right temporal, frontal lobe supplementary cortex, left frontal and little bid left parietal lobe, and bilateral visual cortex. The eyes were open. (Fig: 16, 17, 18). The Left-Hand Finger Taping showed Increased BOLD activity on the right supplementary cortex and right motor cortex. These areas are topographically normal and didn’t affect by stroke (Fig: 19, 20, 21). Speaking tested with repeating a single word during 60 sec, 30 sec. Active 30 sec. Rest period. It takes 4 min. There was a high degree of BOLD activity on the right frontotemporal area. The eyes were open. From this, the occipital areas showed extra BOLD activity. But this is normal. There is an activity on the basal nuclei bilaterally. It was not explained (Fig 22). After 11 months of the therapy, right-hand finger taping showed increased activity in the right motor and premotor cortical areas. But this activity is less than before (see Fig. 16,17,18) (Fig 23,24,25). After 11 months of the therapy, left-hand finger taping showed increased activity on the right motor cortex. This activity has not changed (see Fig. 19,20,21) (Fig 26,27,28). Right Hand Sensorial investigation showed activity on the left parietal cortex, and right motor cortex (Fig 29,30,31,32). The tongue movements showed increased BOLD activity on the prefrontal area, right temporal lobe, and basal nuclei (see fig 22) (Fig 33, 34, 35). The fMRI showed increased BOLD (Blood Oxygen Level Dependence) activity after right-hand finger taping on the right premotor cortex. After 8 months right-hand movements showed newly organized areas on the right cortex.
Table 1: MRC Scale of Results





Conclusion:
We used the Mentamove® method which is registered as a Brain Efficiency Training on our subject continually for 5 months. We didn’t see any complications or side effects in this case. Clinically in the first three weeks, the patient showed some positive developments in his mind and reduced spasticity in his arm. These were are showed by photos (Fig 6,7,8,9,10). The reduction of spasticity with this method showed by C. Crisan at.( 2001) (1).
The method is applied from the shoulder to the wrist extension. This progress is used with our experiences and our opinion based on the brain cortex organization as a homunculus. The patient increased his arm activity dramatically over five months (Table 1 and Fig 11,12,13,14,15). Surprisingly his recalling problems and cognitive functions showed improvement. Sometimes he began to use his right hand spontaneously to take a glass of water. These dramatic activities were seen clinically. But not investigated with fMRI before or after this method’s application. Witte (1998) wrote about lesion-induced brain plasticity and potential mechanisms for recovery (2). And the Mentamove® method is based also on the brain reorganization theory (3). The brain reorganization theory is based on neuroplasticity. The main idea of this theory is ‘’If is there a true method for training the brain can be reorganized itself’’.
We investigated the subject brain activity with 1.5 Tesla MRI (GE Signa Model 2002). After the 5th month and 11th months of the therapy. After 5 months of the therapy, fMRI showed high-level BOLD activity on the right frontotemporal and premotor cortices (Fig 16, 17, 18) with right-hand finger taping. On the other hand, the left-hand finger taping showed less BOLD activity (Fig 19, 20,21) than the right hand on the right motor cortex (Fig 19,20,21). The motor cortex of the left hand was not changed but the right-hand activities were transferred to the right hemisphere. It was surprisingly interesting. Because the left hemisphere premotor cortex was unaffected totally by ischemia. And the other side the talking showed a right temporal and premotor cortex activity during the repeat of a word (Fig 22). At the 11th month of therapy, these findings showed again on the right hemisphere during right-hand finger taping (Fig 23,24,25) and with left-hand finger taping (Fig 26,27, 28). The sensational examination of the right hand showed also right premotor cortex activity in the 11th month. And the last examination with fMRI of the tongue movements showed a right temporal, frontal increased cortical activity (Fig 33,34,35). All these data are very interesting because didn’t explain before using this method. These results show increased activity on the right hemisphere during training with the Mentamove® Method, and newly reorganized areas after the therapy. The fMRI supports the reorganization theory of the brain after ideomotor training due to neuroplasticity.
Abstract ID: A0161
The Mentamove® Rehabilitation After Left Carotid Artery Occlusion: fMRI Findings after Treatment (Case Report)
M. Akgun1, B. Hakyemez2, Z. Akgun3, C. Garner4
1State Hospital of Bursa Neurosurgery MD, TURKEY, 2 State Hospital of Bursa Radiology MD, TURKEY, 3 Uludag University School of Health Ph.D., TURKEY, 4 KWA Clinic Stift Rottal Neurology and Neurorehabilitation MD, GERMANY
Background: Brain Efficiency Training (Mentamove®) is a neurorehabilitation method used for rehabilitation after various brain lesions. If the motoric activities are mentally practiced by the patient, the real movement gives a reorganization to the brain.
Methods: Our case (a 53-year-old, left-handed male) had left carotid artery occlusion. He still displayed right-side spastic hemiparesis 15 months after the stroke, with motor dysphasia and cognitive recall problems. The Mentamove® training program was applied only on the right arm 1 time/daily. The results were measured with the Medical Research Council Scale (MRC) of 0-5 and video documentation. The resulting brain activity was investigated with fMRI after 3 months, and 8 months after the use of the Mentamove® treatment.
Results: Using the MRC scale, the motor power increased on the right shoulder abduction from 3 to 5, and the elbow extension improved from 2 to 5. The wrist extension improved from 0 to 4.
The fMRI showed increased BOLD (Blood Oxygen Level Dependence) activity after 2 months of the Mentamove® therapy, with right-hand movements on the right premotor cortex. After 8 months right-hand movements showed newly organized areas on the right cortex.
Conclusion: These results show increased activity on the right hemisphere during training with the Mentamove® Method, and newly reorganized areas after the therapy. The fMRI supports the reorganization theory of the brain after ideomotor training.
Refferences
- R. Crisan, C. Garner: Effectiveness of EMG-initiated muscular stimulation in outpatients one year post-stroke Neurologie & Rehabilitation 6/2001, Hippocampus Verlag, ISSN 0947-2177, S. 228-232.
- Witte OW (1998): Lesion-induced plasticity as a potential mechanism for recovery and rehabilitative training. Curr Opinion Neurol 11, 655-62
- The Guide of the Mentmove® Method. 2000 pIfR Privat-Institut für Reha-Anwendungen GmbH&Co Medizintechnik KG Kastanienweg 33 85757 Karlsfeld
Kaynaklar ve Benzer Vakalar
- https://drmustafaakgun.com/mentamove-ile-rehabilitasyon/
- https://drmustafaakgun.com/the-mentamove-rehabilitation-2/
- https://drmustafaakgun.com/akut-spinal-kord-kompresyonu-sonrasi-paraplejide-mentamove-tedavisinin-etkisi-olgu-sunumu/
- https://drmustafaakgun.com/paraparezi-ve-mentamove/
- https://drmustafaakgun.com/bilateral-distal-paraplejide-mentamove/
- https://drmustafaakgun.com/kafa-travmasi-sonrasi-mentamove/
- https://drmustafaakgun.com/beyin-etkin-calisma-egitimi/
- https://drmustafaakgun.com/mentamove-metodu-ile-rsd-refleks-sempatik-distrofinin-tedavisi/
- https://drmustafaakgun.com/foot-drop-mentamove-metodu/
- https://drmustafaakgun.com/the-mentamove-rehabilitation/
- https://drmustafaakgun.com/the-oculomotor-palsy-after-right-posterior-communicant-aneurysm-surgery-and-treatment-with-mentamove-case-report/
- https://drmustafaakgun.com/mentamove-rehabilitasyon-nedir/
- https://drmustafaakgun.com/category/norolojik-rehabilitasyon/
- https://drmustafaakgun.com/mentamove-tedavisi/