The Mentamove Rehabilitation After Right Total Carotid Artery Occlusion: fMRI Findings After Treatment (Case Report)
Dr. Mustafa Akgün1, Dr. Zehra Akgün2, Dr. Bahattin Hakyemez3, Dr. Christoph Garner4
1 State Hospital of Bursa Neurosurgery MD,Turkey, 2 Uludag University School of Health PhD, Turkey, 3 State Hospital of Bursa Radiology MD,Turkey, 4 KWA Clinic Stift Rottal Neurology and Neurorehabilitation MD, Germany
Keywords: Right Carotid Artery Total Occlusion, Stroke, Hemiparesis, Electromyography, Rehabilitation, Biofeedback, Electrotherapy, Neuroplasticity, Relearning, Brain Efficiency Training, Mentamove®, fMRI
Background
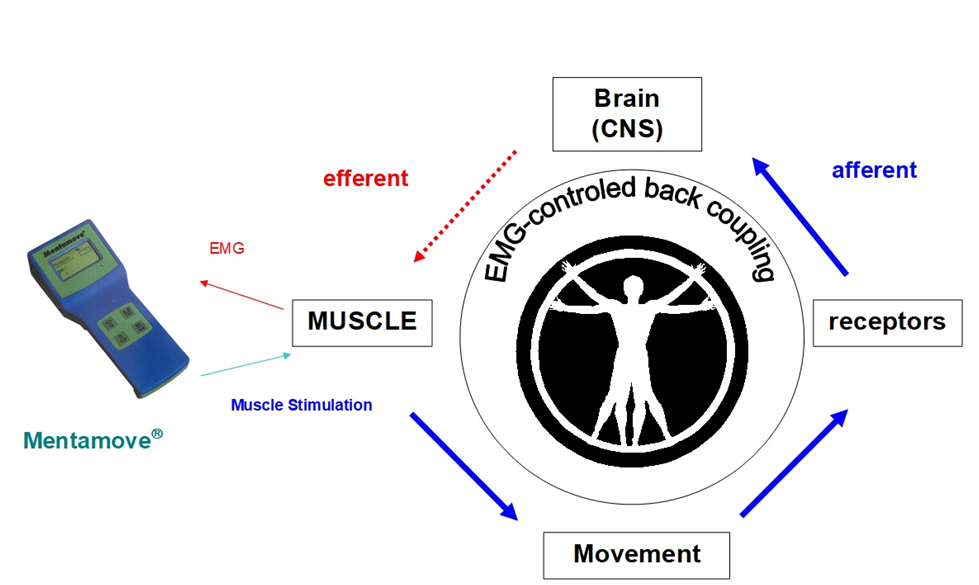
Brain Efficiency Training (Mentamove®) is a neuro-rehabilitation method used for rehabilitation after various brain lesions. If the motoric activities are mentally practiced by the case with Mentamove, the real movement gives a reorginasation to the brain, due to neuroplastisity. EMG-initiated muscular stimulation gives is an effect mainly used in the treatment of stroke patients (1). It is a combination of muscular stimulation with medium frequency sine current and a biofeedback process (Fig 1).
Methods: Our subject (a 50 year old, right handed male) had total right carotid artery occlusion (Fig 2). He had left flask hemiplegia with mild central type fascial paralysis. After 2.5 week hospitalisation, the Mentamove® Method was used on the left shoulder (mm.supraspinatus and deltoideus), elbow (m.triceps brachii), wrist (m.extensor digitorum, m. extansor carpi ulnaris, m.extansor carpi radialis longus and brevis), hip (m. quadriceps femoris), and knee (distal part of m.quadriceps femoris) and peroneal (m.tibialis anterior) muscles 1 time /daily device during a 7 month period. The results were measured with the Medical Research Council Scale (MRC) of 0-5, video documentation and photografic documentation. The brain activity was investigated with fMRI after 7 months, and again 13 months after the inception of the treatment. Every seasons duration was 20 minutes. The case worked totally 7 months.
We investigated the right and left hip flexion/extension movements, righ and left foot dorsiflexion/plantar flexion movements after 7th month of the therapy. At the 13th month of inception of the treatment we inspected the right and left foot dorsiflexion/plantar flexion movements, left elbow flexion/extension movemens, and right/left hand sensorial activity with 1.5 TESLA GE MRI. The movements activity took 30 sec. and rest period took 30 sec. During 8 minutes.

Results and Outcome: The patient begun to work with mentamove® at home. After 7 days he begun to walk with assistance but after 20 days he begun to walk alone but cant move his left arm (Fig 3,4). After 7 days the foley catheter taken out. After 30 days he begun to go to the our outpatient rehabilitation clinic. After 4 months he can walk to the upstairs alone, and he can control left foot rapidly to control a ball (Fig 5,6). And he begun to move the left shoulder to the 90° abduction (Fig 7,8). After 7 months he begun to do extension and flexion left elbow (Fig 9,10,11).
Using the MRC Scale, the motor power of the shoulder abduction, hip flexion, knee extension, dorsiflexion increased from 0 to 5, and the elbow extension from 0 to 4, The wrist extension improved from 0 to 2 (Table 1).
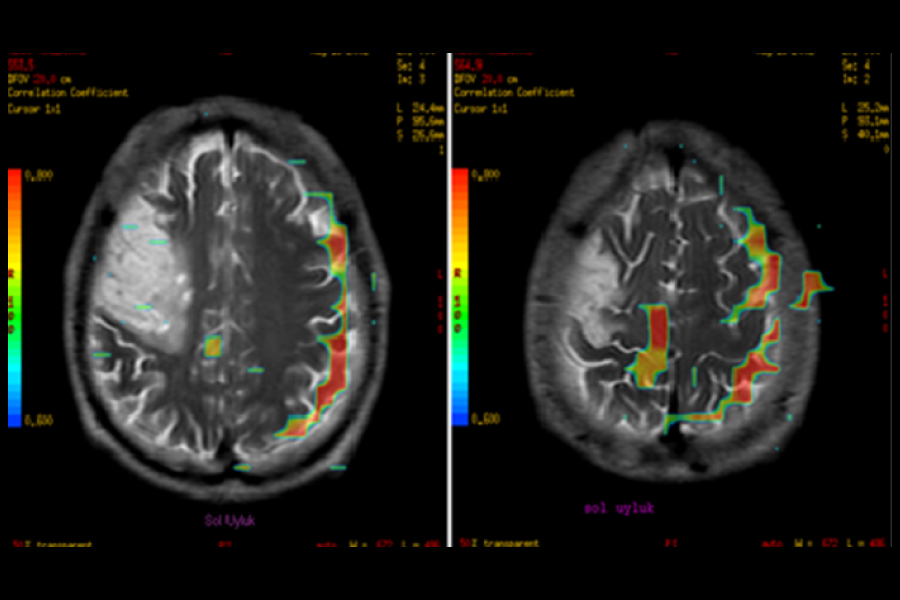
The fMRI showed BOLD (Blood Oxygen Level Dependence) activity after 7 months, diffuse cortical activity during right and left foot dorsiflexion and left hip flexion movements. After 13 months, the left foot dorsiflexion and triceps activity showed new organised areas on the right cortex, these areas were showed on border of the ischeamic zone.
Table 1: MRC Scale of Results












Conclusion
This case invited to work with mentamove® at early period after stroke. The MRI showed sharp infarct area on the right hemisphere and carotid occlusion (Fig 2).
Then he worked with mentamove® his daughter assitence at home during 1 month. After 7 days he begun to walk with assistance but after 20 days without assistance (Fig 3). After 1 month he invited to our outpatient rehabilitation center. There he worked with mentamove® only and walked on upstairs worket for foot movements control itself. In this period he showed shoulder abduction movements, the 90° movement completed after 4 months. Then he worked only on the triceps muscle activity during 2 months (Fig 4,5,6).
When after 7 months the patient stopped working with mentamove®, we decided to exam his brain activity with fMRI technique (we havent 1.5 Tesla fMRI device before this time). This was our first fMRI investigation after mentamove treatment, then we decided to investigate the right side functions for control.
Our first investigation begun from right hip flexion/extension activities (Fig 7). In first step it surprised us because it showed frontal lobe, lymbic system activity impressively. It was a BOLD activity of working memory. It may be a wrong from patients emotion and concentration mistake at this time. But we didn’t deleted these images and showed here. Because some reasearches investigated the working memory and showed same BOLD activity. Interestingly the motor cortex of the right hip not showed high level BOLD activity (Fig 7). In the second step we investigated the left hip flexion/extension, the right motor cortex of the leg showed BOLD activity and the surfase of the posteior parietal cortex, and premotor cortex of frontal lobe (Fig 8).These are diffuse activities on the contrlateral sensorimotor cortex. These BOLD activities may be combined with right motor cortex activity of left leg (2,3).
The right foot dorsflexion/plantar flexion actvities investigated with fMRI (Fig 9) and left foot (Fig 10). The right foot showed and BOLD activity on the right and left motor cortex of leg and diffusely on the left hemisphere surface (Fig 10). Same findings showed with left foot motor activities ont the left motor cortex and left cerebral hemisphere surface. These BOLD activities are more than rihgt foot movements (Fig 10). The increased BOLD activity on whole hemisphere for each movements may be due to the increased mental concentration and thinking. Because there are many working cortical areas at the same time (2,3). These findings investigated after 6 months when the therapy stopped.
13th month of the therapy the patient investigated with fMRI for triceps muscle activity bilaterally (Fig 11,12), right and left foot dorsiflexion/plantar flexion bilaterally (Fig 13, 14) and right hand, and left hand sensorial drawing bilaterally (Fig 15,16).
At the Fig 11, the right triceps activities showed BOLD activity on the left motor cortex and right premotor cortex. The right premotor cortex combined with left motor cortex for doing this movement (Fig 11). The left triceps activities showed an increased BOLD activity on the right premotor cortex ant right hemisphere surface, but interestingly the border of the iscaemic zone shoved high level BOLD activity. It combined with motor cortex activities. These area works for left triceps movements (Fig 12).
At the Fig 18, 19 we investigated the right foot and left dorsiflexion/plantar flexion activities. The right foot motor movements increased the BOLD activity on the prefrontal, frontal cortex, lymbic system, left hippocampus, left temporal lobe, and little bid at the left motor cortex. The left foot movements increased BOLD activity on the right cerebellum, right frontal cortex, right premotor and motor cortex and the borders of ischaemic zone (Fig 19). These activities are less than 6 months ago (Fig 16) these well done with little mental effort.
At the Fig 15, 16 we investigated the right and left hand sensorial condition with drawing hand inner surface. The right hand sensorial activities showed on the left sensorimotor cortex (Fig 15) but the left hand drawing showed the BOLD increased activity on the right frontal cortex and right hippocampus (Fig 16).
These results demonstrate increased activity of the whole hemisphere during training with the mentamove® Method, and newly reorganised areas after the therapy. The fMRI supports the reorganisation theory of the brain after ideomotoric training.
Refferences
- R. Crisan, C. Garner: Effectiveness of EMG-initiated muscular stimulation in outpatients one year post-stroke Neurologie & Rehabilitation 6/2001, Hippocampus Verlag, ISSN 0947-2177, S. 228-232.
- H. Kondo, M.Morishita, N. Osaka, M. Osaka, H. Fukuyama, and H. Shibasaki: Functional roles of the cingulo-frontal network in performance on working memory; NeuroImage 21 (2004) 2 – 14
- Timothy P. L. Roberts and Howard A. Rowley, Mapping of the Sensorimotor Cortex: Functional MR and Magnetic Source Imaging AJNR Am J Neuroradiol 18:871–880, May 1997
Abstract ID: A0155
The Mentamove Rehabilitation After Right Total Carotid Artery Occlusion: fMRI Findings After Treatment (Case Report)
Dr. Mustafa Akgün1, Dr. Zehra Akgün2, Dr. Bahattin Hakyemez3, Dr. Christoph Garner4
1 State Hospital of Bursa NeurosurgeryMD, Turkey, 2PhD Uludag University School of Health , Turkey, 3 State Hospital of Bursa Radiology MD,Turkey, 4 KWA Clinic Stift Rottal Neurology and Neurorehabşlitation MD, Germany
Background: The Brain Efficiency Training (Mentamove) is a neuro-rehabilitation method used for rehabilitation after various brain lesions. If the motoric activities are mentally practised by the case with Mentamove, the real movement gives a reorginasation to the brain, due to neuroplastisity.
Methods: Our subject (a 50 year old, male) had total right carotid artery occlusion. He had left hemiplegia with mild central type fascial paralysis. After hospitalisation, the Mentamove Method was used on the left shoulder, elbow, wrist, hip, and knee and peroneal muscles 1 time /daily device during a 7 month period. The results were measured with the Medical Research Council Scale (MRC) of 0-5, and the brain activity was investigated with fMRI after 7 months, and again 13 months after the inception of the treatment.
Results: Using the MRC Scale, the motor power of the shoulder abduction, hip flexion, knee extension, dorsiflexion increased from 0 to 5, and the elbow extension from 0 to 4, The wrist extension improved from 0 to 2. The fMRI showed BOLD (Blood Oxygen Level Dependence) activity after 7 months, diffuse cortical activity during right and left foot dorsiflexion and left hip flexion movements. After 13 months, the left foot dorsiflexion and triceps activity showed new organised areas on the right cortex, these areas were showed on border of the ischeamic zone.
Conclusion: These results demonstrate increased activity of the whole hemisphere during training with the Mentamove Method, and newly reorganised areas after the therapy. The fMRI supports the reorganisation theory of the brain after ideomotoric training.
Kaynaklar ve Benzer Vakalar
- https://drmustafaakgun.com/mentamove-ile-rehabilitasyon/
- https://drmustafaakgun.com/the-mentamove-rehabilitation-2/
- https://drmustafaakgun.com/akut-spinal-kord-kompresyonu-sonrasi-paraplejide-mentamove-tedavisinin-etkisi-olgu-sunumu/
- https://drmustafaakgun.com/paraparezi-ve-mentamove/
- https://drmustafaakgun.com/bilateral-distal-paraplejide-mentamove/
- https://drmustafaakgun.com/kafa-travmasi-sonrasi-mentamove/
- https://drmustafaakgun.com/beyin-etkin-calisma-egitimi/
- https://drmustafaakgun.com/mentamove-metodu-ile-rsd-refleks-sempatik-distrofinin-tedavisi/
- https://drmustafaakgun.com/foot-drop-mentamove-metodu/
- https://drmustafaakgun.com/the-mentamove-rehabilitation/
- https://drmustafaakgun.com/the-oculomotor-palsy-after-right-posterior-communicant-aneurysm-surgery-and-treatment-with-mentamove-case-report/
- https://drmustafaakgun.com/mentamove-rehabilitasyon-nedir/
- https://drmustafaakgun.com/category/norolojik-rehabilitasyon/
- https://drmustafaakgun.com/mentamove-tedavisi/