Dikkat: Sitemizde yayınlanan bazı bilgiler dış kaynaklardan alınmıştır. Bu kaynaklara doğrudan link verilmektedir. Pasaj sonundaki literatür bilgileri dışında başka sitelere çıkış yapma olasılığınız vardır. Tekrar geri dönmek için ilgili siteye gitmek istediğinizde yeni sekme açarak gitmeniz daha uygun olur. Doğrudan dış sitelere gittiğinizde geri dönmek isterseniz adres çubuğundan geri tuşu ile tekrar bu metne dönebilirsiniz.
Aynı şekilde başka sitelerde yayınlanmış görsellere de ulaşmak için kaynağına gidebilirsiniz. İlgili görseli kaynağında ziyaret edebilirsiniz.
Sitemizde bize ait görüntüler herhangi bir telif hakkı talep edilmeksizin kopya edilebilir, kullanılabilir. Kaynağın bizim sitemiz olduğunu belirtmeniz yeterlidir.
Sitemiz bilgilendirme amaçlıdır. Sitemize herhangi bir reklam uygulaması alınmamaktadır. Sitemiz bilgi paylaşım amaçlı olup, tıp ile ilgilenen herkese açıktır. Üyelik zorunlu değildir.
Hazırlanan içeriklerimiz tamamen amatör ruhla hazırlanmakta olup, aynı şekilde video kanalımız linki.
https://www.youtube.com/channel/UC3JBKVVaVfhI1z_rKMDUuZg/
Video kanalımız üzerinden bizi takip edebilir, abone olabilir, bize mesaj bırakabilirsiniz. Yorum bırakmanız halinde hatalarımızı düzeltmek için güncel olmamıza katkı sağlayabilirsiniz.
Tüm takipçilerimize teşekkür ederiz.
Last Revision: 02.12.2022
The Oculomotor Palsy After Right Posterior Communicant Aneurysm Surgery Treatment With Mentamove (Case Report).
Z. Akgun1, M. Akgun2, C. Garner3
1 Uludag University School of Health PhD, TURKEY, 2 State Hospital of Bursa Neurosurgery MD, TURKEY, 3 KWA Stift Rottal Clinic Neurology and Neurorehabilitation MD, GERMANY
Keywords: Subarachnoid Haemorrhage, Posteior Communicant Artery Aneurysm, Aneurysm Surgery Complications, Ptosis, Occulomotor Nerve, Oculomotor Nerve Rehabilitation, Electromyography, Rehabilitation, Biofeedback, Electrotherapy, Neuroplasticity, Brain Efficiency Training, Mentamove®
| Abstract ID: A0153The Occlomotor Nerve Palsy After Right Posterior Communicant Aneurysm Surgery And Treatment WithMentamove® (Case Report)Dr. Zehra Akgün1, Dr. Mustafa Akgün2, Dr. Christoph Garner3 1 Uludag University School of Health PhD, TURKEY, 2 State Hospital of Bursa Neurosurgery MD, TURKEY, 3 KWA Stift Rottal Clinic Neurology and Neurorehabilitation MD, GERMANY Web: www.mentamove.com.tr e-mail: info@mentamove.com.tr Background: The “Brain Efficiency Training” Mentamove® is a neurorehabilitation method is used for the rehabilitation after various brain lesions. If the motoric activities are mentally practised by the case, the real movement gives a reorginasation to the brain due to neuroplastisity. But never have been used at the periferic nevre lesions before. Methods: The present case (42 years old female) operated for right posterior communicant artery aneurysm. After operation she showed right side ptosis, occulomotor nerve palsy with diplopia and pupil dilatation and left side central type fascial paralysis. The Mentamove® Therapy applied on the right m. palpebrae superior and m. frontalis, and for left fascial muscles 1 time/daily. The outcome monitorised by photos. Results: After 2 weeks she begun slightly open the right eye. After 4 weeks she opened the right eye totally but couldn’t look to medial side. We suggested for practice for look to nose mentally 20 times/dailiy without Mentamove®. After 6 weeks she recovered totally, the pupill, diameters and reactions showed total recovery. Left side fascial paralysis recovered after 6 week of the therapy.Conclusion: These data showed a new idea to threat the peripheric nerve lesion deficits with Mentamove® after incompelete injury of the nerves. |
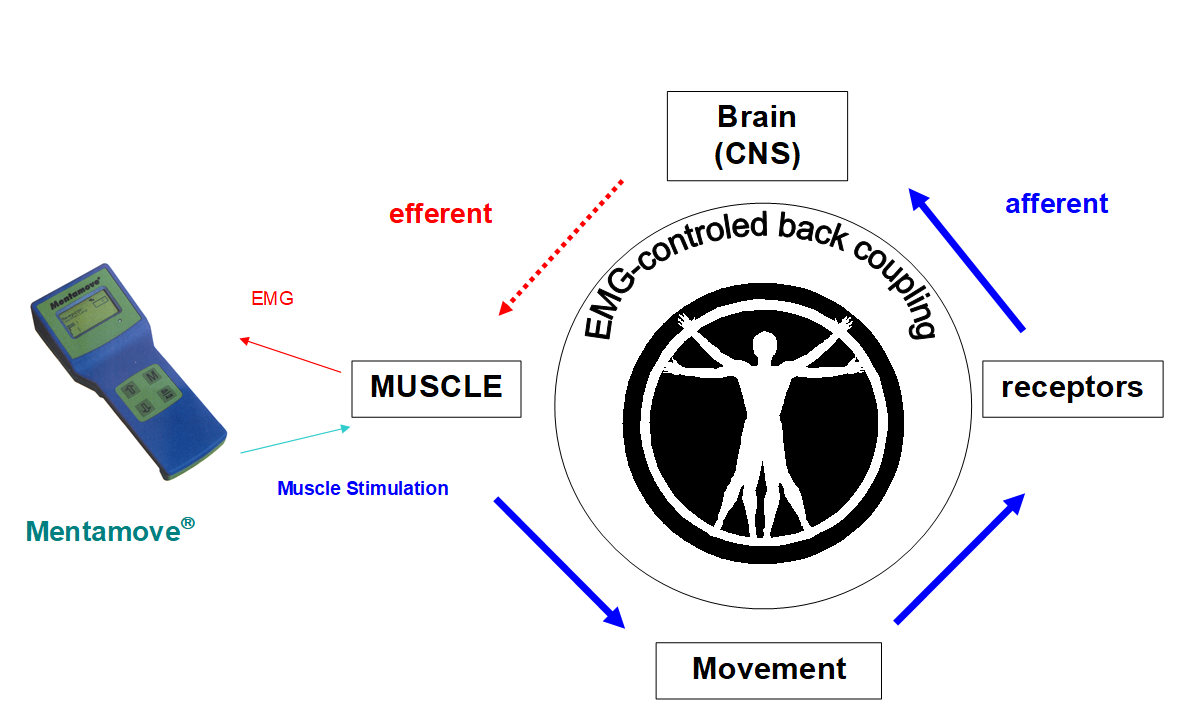
Background: The “Brain Efficiency Training” Mentamove® is a neurorehabilitation method is used for the rehabilitation after various brain lesions. If the motoric activities are mentally practised by the case, the real movement gives a reorginasation to the brain due to neuroplastisity. EMG-initiated muscular stimulation gives is an effect mainly used in the treatment of stroke patients. It is a combination of muscular stimulation with medium frequency sine current and a biofeedback process (Fig 1). But never have been used at the periferic nevre lesions and cranial nerve lesions before. Our opinion comes from the biofeedback coupling theory and if is the method works trully it may be give the positive effect like central nervous system for recovery. The efferent and afferent ways of the cranial nerves work differently from other peripheric nerves. The motor fibers (efferent) of the m. palpebrae sup. have two ways N. Oculomotorius (III) (Fig 2) and Cervical Sympathetic Chain (Sup. Cervical Ganglion) (Fig 3). The M. Orbicularis Oculi and M. Fontalis innervates with efferent fibers of the N. Fascialis (VII), this cranial nerve comes from the facial motor nuclei of the brain stem. The Oculomotor nerve also carries the motor (efferent) fibers to the (m.rectus medialis, m. sphincter pupilla) from nuclei of the brain stem and mesensephalon. These nuclei are under the mental motor control of the temporal (fascial) and frontal (eye conjugated movements) lobes bilaterally. But the sensorial ways (afferent) works with N. Trigeminus (V) and its sensorial nucleus is in the brain stem. Our theory bases on the incomplete motor oculomotor nerve fibers injury and healthy trigeminal nerve fibers. The parasympathetic (efferent) fibers come with oculomotor nerve to the ciliary ganglion and to the sphincter pupilla. These fibers placed superficially on the III. Nerve. When the nerve affected partially or totally the pupilla dilatation and ptosis were seen. If the injury affects the deep fibers of the III. nerve the medial rectus have been paralysed. It is urgent for intracranial surgical decompression (1, 2, 3). There is no prior documented case treating on the cranial nerve lesions with Mentamove®. But our opinion comes from the biofeedback coupling theory and if is the method works trully it may be give the positive effect like central nervous system for recovery (Fig 1). Sometimes a big aneurysm on the posterior communicant artery may compress the III. nerve, this clinical data may be seen spontaneously. Also during the surgical procedures for these aneurysms the III. nerve may be injured.
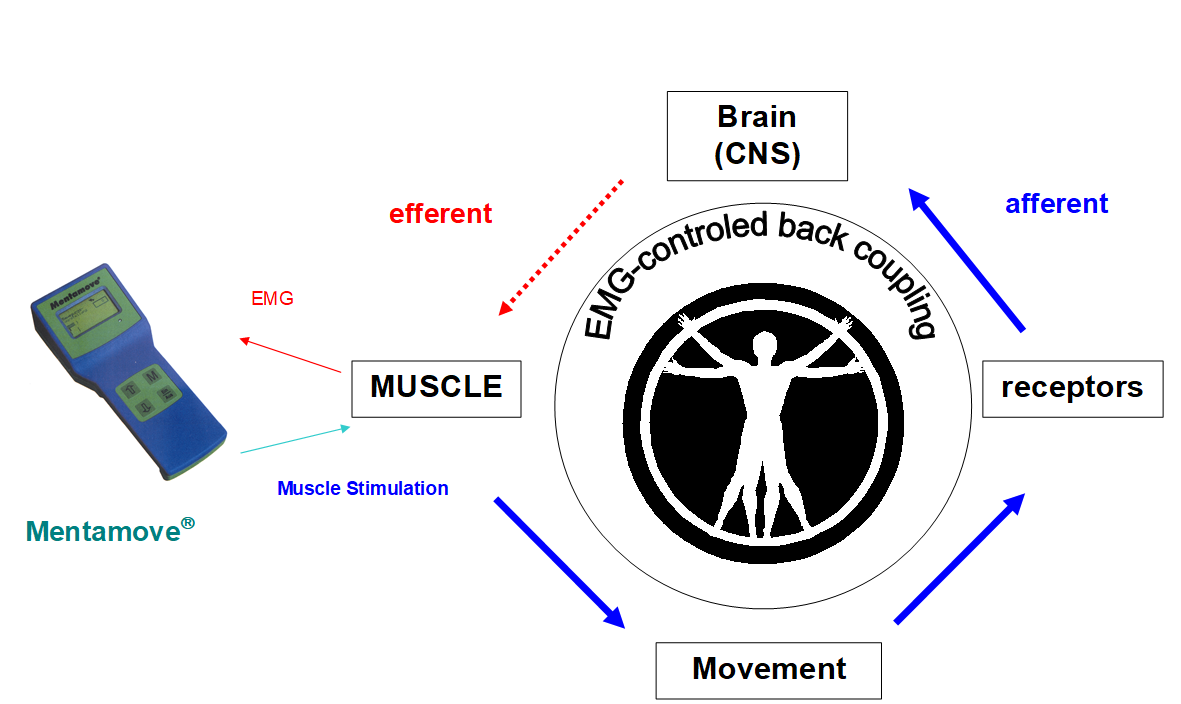

Fig 2: The oculomotor nerve motor and parasymphathetic ways, (Fitzgerald et all)

Fig 3: The sympathetic control and ways of the Levator Palpebrae and Dilatator Pupilla. (Fitzgerald et all)
Methods: The present case (42 years old female) operated for right posterior communicant artery aneurysm (Fig 6,7,8) after subarachnoid haemorrhage (Fig 4,5). Our surgical approach was; right side pterional craniotomy, dural opening, sylvian arachnoid dissection, carotid cistern dissection and right posterior communican artery aneurysm dissection under surgical microscope. During this dissection of the aneurysm we used temporary clip application on the right carotid artery. During dissecting aneurysm the right oculomor nerve visualised, and there was used a bipolar coagulation for some hemorhagies from cavernous sinus and dura. During this coagulation the III. Nerve moved slightly. Aneurysm clipped. After operation she showed the right side ptosis, occulomotor nerve palsy with diplopia and pupil dilatation, medial rectus and left side central type fascial paralysis (Fig 11). The postop control CT was normal after operation (Fig 9,10). In the first time we tried to apply electrodes of mentamove® on the right frontalis muscle to see the EMG signals. There was a 8-10 μv EMG amplitude signals. Then we tried to measure the same signals from the upper eye lip, and we measured about 7-8 μv. Then we tried with 2 μv offsett value for triggering EMG stimulation. After 1course investigation we decided to survive the treatment. Because there we measured max contraction activity and increased offset value from 2 μv to 4 μv. The Mentamove® Therapy applied on the right m. palpebrae superior, m.orbicularis oculi and m. frontalis, and for left fascial muscles 1 time/daily. The outcome monitorised by photos.The treatment completed after 20 days (=20 seasons). After therapy the right palpebral elevation completed and normal view of the eyes was seen. But the midriasis and the medial rectus plegia was not improved. Then we suggested another practise to look to the apex of nose without electrostimulation. This practice continued during 2 weeks about 20 times/dailiy. Every step of recovery ducemented by photos.

Fig 4,5: Subarachnoid Haemorrhage in the right quadrigeminal cisterna.
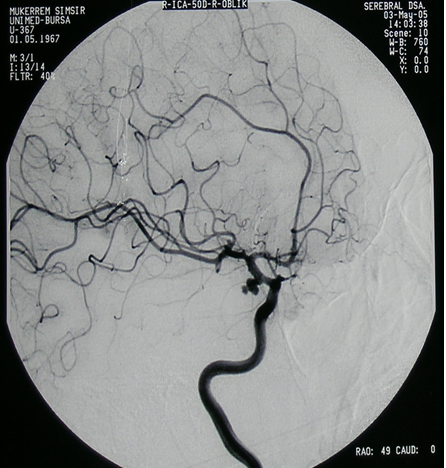


Fig 6,7,8: Saccular aneurysm on the right post. Communicant artery and carotid artery bifurcation
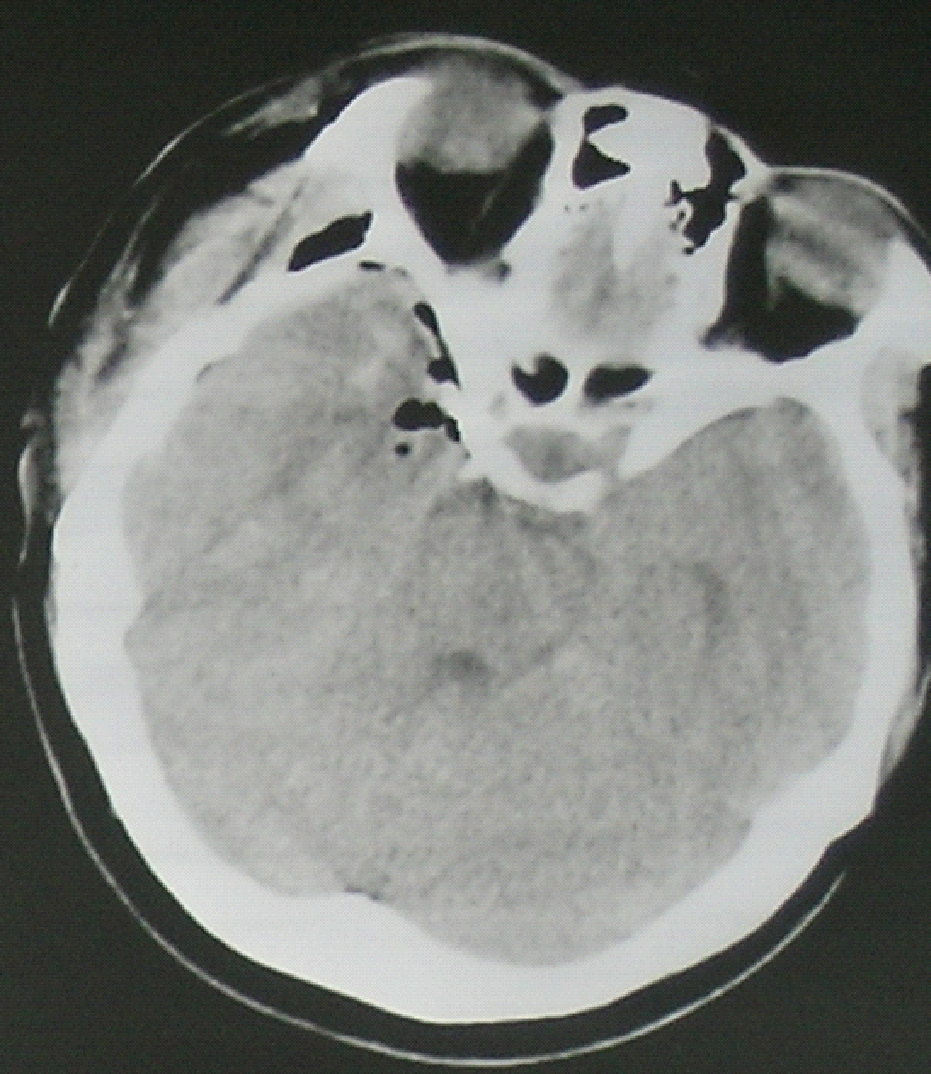

Fig 9,10: Postoperative control CT shows an artefact of clip on clipped aneurysm.
Results: After 2 weeks she begun to open the right eye slightly. After 4 weeks she opened the right eye totally but couldn’t look to medial side (fig 12, 13). We suggested for practice for look to nose mentally 20 times/dailiy without Mentamove®. After 6 weeks she recovered totally, the pupill, diameters and reactions totally improved.

Conclusion
The oculomotor nerve my be injured during aneurysm surgery. The bipolar coagulation, dissection the aneurysm traction of the dome are causes of the oculomotor nerve injury. These manipulations may injured the oculomotor nerve incompletely.
After clinical examination we tested the patient first time with Mentamove® device and decided to achieve method. The m. frontalis, m. orbicularis oculi, m. palpebra superior 1 course daily. After two weeks she showed slightly open the right eye (Fig 12). We survived the therapy to three weeks. After 20 course of the therapy she opened the right eye totally, but the pupil diameter was 4 mm, and didn’t show any reaction to light. And the was deviated laterally due to the medial rectus plegia. Then we hypothesised a theory while the mentamove working the patient tries to open the eye. So the patient now may trie this training without stimulation. Because we have not a muscle on the pupil contraction for stimulation, and it was not possible stimulate the m.rectus medialis with EMG triggering. But practically the pupil goes to the contraction while looking to the short distance like tip of nose. During this exercise m. rectus medialis also does contraction for move medially the eye globe conjugately. We aimed to take a benefit from this activity for threat this weakness of pupil and m.rectus medialis. While beginning an improvement survive of the eye palpebral activities we combined a new training exercise with phisiological ways. After 2 weeks of these exercise program the patient completed her eye mevements activities and pupil contractions by reflex mecanisms. This approach is same as mentamove training without muscle stimulation bases on the biofeedback principles.
These data showed a new idea to threat the incompletelly injured peripheric and cranial nerve lesion deficits with Mentamove® after incomplete injury of the nerves.
Literature
- R. Crisan, C. Garner: Effectiveness of EMG-initiated muscular stimulation in outpatients one year post-stroke Neurologie & Rehabilitation 6/2001, Hippocampus Verlag, ISSN 0947-2177, S. 228-232.
- P. Williams, W. Warwick, M.Dyson, L.Bannister: Gray’s Anatomy: The Cranial Nerves; pp:1096-1098 37th Edition, Churchill Livingstone, New York 1989.
- M.J.T. Fitzgerald, J.Follan, J.Curran; Clinical Neuroantomy and Related Neruoscience: Ocular Motor Nerves pp:187-193. Fourth Edition, W.B.Saunders, Harcourt Publishes Ltd. London, 2002
Kaynaklar ve Benzer Vakalar
- https://drmustafaakgun.com/mentamove-ile-rehabilitasyon/
- https://drmustafaakgun.com/the-mentamove-rehabilitation-2/
- https://drmustafaakgun.com/akut-spinal-kord-kompresyonu-sonrasi-paraplejide-mentamove-tedavisinin-etkisi-olgu-sunumu/
- https://drmustafaakgun.com/paraparezi-ve-mentamove/
- https://drmustafaakgun.com/bilateral-distal-paraplejide-mentamove/
- https://drmustafaakgun.com/kafa-travmasi-sonrasi-mentamove/
- https://drmustafaakgun.com/beyin-etkin-calisma-egitimi/
- https://drmustafaakgun.com/mentamove-metodu-ile-rsd-refleks-sempatik-distrofinin-tedavisi/
- https://drmustafaakgun.com/foot-drop-mentamove-metodu/
- https://drmustafaakgun.com/the-mentamove-rehabilitation/
- https://drmustafaakgun.com/the-oculomotor-palsy-after-right-posterior-communicant-aneurysm-surgery-and-treatment-with-mentamove-case-report/
- https://drmustafaakgun.com/mentamove-rehabilitasyon-nedir/
- https://drmustafaakgun.com/category/norolojik-rehabilitasyon/
- https://drmustafaakgun.com/mentamove-tedavisi/