Mentamove Metodu, bu vaka raporundan önce Kauda Ekina Sendromu (CES) eksikliklerinin ve paraplejinin tedavisinde kullanım için hiçbir zaman belgelenmemiştir.
Dr. Christoph Garner1, Dr. Mustafa Akgün2, Dr. Zehra Akgün3
1KWA Stift Rottal Neurology and Neurrehabilitation MD, Germany, 2 State Hospital of Bursa MD Neurosurgery,Turkey, 3 Uludag University School of Medicine PhD, Turkey
Keywords: Cauda Equina, Cauda Equina Syndrome, Lumbar Compression Fracture, Paraplegia, Urinary Retention, Priapism, Electromyography, Rehabilitation, Biofeedback, Electrotherapy, Brain Efficiency Training, Mentamove®, Neuroplasticity, Relearning
Background: Brain Efficiency Training (Mentamove®) is a neurorehabilitation method used for rehabilitation after various brain lesions. If the motoric activities are mentally practiced by the patient, the real movement gives a reorganization to the brain, due to neuroplasticity. EMG-initiated muscular stimulation gives is an effect mainly used in the treatment of stroke patients (1,2,3). It is a combination of muscular stimulation with medium-frequency sine current and a biofeedback process (Fig 1). The Cauda Equina Syndrome is a syndrome of the distal part of the spinal cord at the level L1-5. The pathology may be a trauma, intervertebral disc degeneration, intradural or extradural tumor, and other masses. Chronically affected spinal caudal fibers can’t control the muscles and muscles show atrophy down at the affected level. The Mentamove® Method has never been documented for use in the treatment of Cauda Equina Syndrome (CES) deficits and paraplegia before this case report.

Methods: The subject of this case (a 30-year-old male) was operated on for an L2 compression fracture (Fig 1,2,3,4,5,6,7,8,9), 3 days after sustaining the injuries in a traffic accident. The spinal surgery used was a complete laminectomy of L2 and L3, and then the Cauda Equina was decompressed (Fig 10,11). The dura was ruptured approximately 4-5 cm and some caudal fibers were disrupted. After dural repair, the posterior spinal instrumentation was implemented (Fig 12,13,14). The subject had total paraplegia before and after surgery, and anesthesia was below the L1 segment. The anal tonus was lost and priapism was noted. After 5 days of the surgical decompression, the Mentamove® treatment program was implemented. Mentamove® was applied to the hip flexors (m quadriceps femoris proximally), knee extensors (m. quadriceps femoris), peroneal group muscles (m. tibialis anterior), gluteal muscles (m. gluteus maximus) and the hamstring muscle groups 2 times/daily bilaterally. The data was measured with the Medical Research Council Scale (MRC) 0-5 and documented photographically. The duration of therapy is 4 months for the right leg and 8 months for the left leg.

Fig 1, 2: X Ray’s show L2 compression fracture

Fig 3,4: CT Shows bone deplacement into the spinal canal

Fig 5,6,7,8,9: MRI Shows the cauda aquina copression by the fractured L2 vertebrae.

Fig 10,11: Postoperative MRI shows decomressed the spinal canal and cauda equina.

Fig 12,13,14: The subject shows no movement on the leg and foots, he meets for first season with. mentamove He begun work alone with mentamove.
Table 1: MRC Scale of Results
| MRC Point Before Treatment | MRC Point After Treatment | |
| Hip Flexion R/L | 0 / 0 Point | 5 / 5 Point |
| Hip Extension R/L | 0 / 0 Point | 5 / 5 Point |
| Knee Flexion R/L | 0 / 0 Point | 5 / 4 Point |
| Knee Extension R/L | 0 / 0 Point | 5 / 4 Point |
| Foot Dorsiflexion R/L | 0 / 0 Point | 5 / 4 Point |
| Foot Plantar Flexion R/L | 0 / 0 Point | 5 / 4 Point |
| Sensorial Deficit R/L | Lower of L1 / Lower of L1 | L3 Hypoesthasia/ L4,5 Hypoesthasia |
| DTR | Absent/Absent | Absent/Absent |
| Chlonus | None / None | None / None |
| Babinski Sign | Unresponsive / Unresponsive | Flexor / Flexor |
| Priapism | Yes | None |
| Anal Tonus | None | Yes |
| Urinary Retension | Yes | None (USG) |
| Reflex Sympathetic Signs | None | None |
Results
After 10 days, the subject was able to slightly move the toes on his right foot. Based on the MRC scale, after 30 days, he started to move the right leg from 0 to 4 (Fig 15). And his left hip demonstrated 2-point muscle activity (Fig 16) internal adductor began to move actively (Fig 16,17), and his left foot showed 2-point motor activity. After 50 days of therapy, he started to stand with assistance. After 4 months of therapy, he walked with 5 points for some muscle control of the legs. He was able to control urinary incontinence and anal tonus. The results are shown in Table 1 and Fig

Fig 15: Video After 30 days, hips flexion and plantar flexions.

Fig 16: After 30 days, adduction.
Fig 17: Video. Starting Bycicle Training after 30 Days of the Mentamove Treatment

Fig 18: Walking on treadmil. After 8 months.
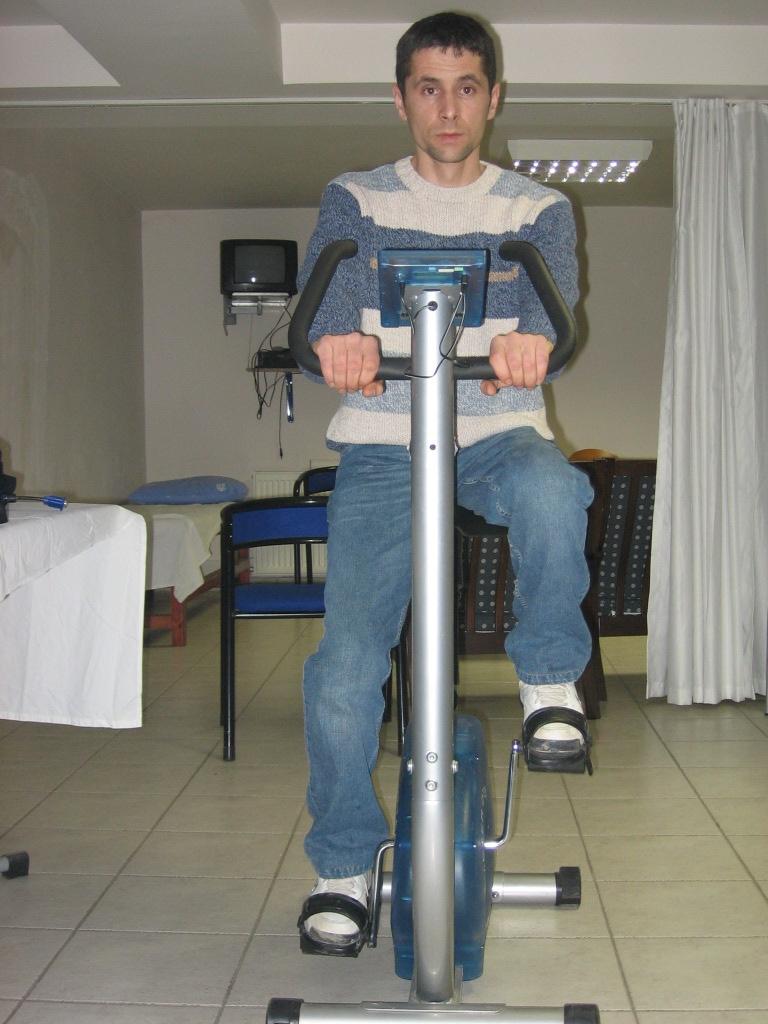
Fig 19: Working on bycicle, after 8 months

Fig 20: Walking on the on the floor, after 8 months of therapy

Fig 21: Walking on upstairs after 8 months of therapy

Fig 22: Walking on upstairs after 8 months of therapy
Conclusion
This case operated for L2 compression fracture on the 3rd day after trauma. The first neurologic signs showed Acute Cauda Equina Syndrome signs. The surgical procedure was applied for decompression of Cauda Equina and stabilization of fractured vertebrae. Spine Surgery aims to earn time for rehabilitation. In this case, we saw the dural laceration and some of the Cauda Equina fibers injured. These fibers can’t be repaired surgically. Only the dura was repaired for CSF fistula.
After stabilization, we tried to measure the EMG signals from peroneal muscles with a surface electrode of mentamove®. This is our test approach for many cases. If the case shows increasing EMG amplitude signals on any muscle then we can stimulate it and we can work for the biofeedback process. This case showed 2 μv EMG activities on the peroneal and quadriceps femoris bilaterally. After this test measurement, the mentamove® therapist applied the procedure on the hip, peroneal, hamstring, and gluteal muscles 2 times daily. In the first 10 days, the case showed little activity to the toe on the right foot. And some sensational feelings began on the level L2,3 bilaterally. After the first 10 days, the patient was discharged from the hospital for self-training at home (Fig 12,13,14).
And then after the second 10 days, he was examined again. His activities increased on the right and left totally, and the left showed increased activity proximally (Fig 15,16,17). And sensational feeling increased from level L3 to the L4,5 dermatome. The signs of Reflex Sympathetic Syndrome were none. He showed turning on the bed alone, but can’t sit alone. When he began to move his legs proximally he increased these activities with self-training in the bed.
He was examined again on the 50th day of the treatment. At this time the foley catheter took out. The urinary retention and voiding were inspected. He didn’t show urinary retention, he can urinate with Crede Maneuver. This condition was inspected for 24 hours. On this day he could urinate 3 times. Then the catheterization was not implemented again. After 3 weeks the ultrasound not showed any urine retention in the bladder. In this period all activities began. In the first week, his sensation was little during coitus, but ejaculation was normal, after 3 weeks he showed great improvement in this.
On the 50th day of therapy, the case was able to stand with assistance. But walking was not enough. Only standing exercised with assistance.
On the 70th day, he began to walk with assistance. Then he has begun to work with the treadmill and bicycle. Every active exercise was implemented when he has begun to use his muscle on the legs.
In all this, during 8 months period, the patient worked at home with mentamove®, and he was examined every 10 days in the first 2 months. After the eve examined every 30 days.
He returned to his old job after 8 months (Fig 18,19,20,21,22).
Our data and the outcome of the patient showed clinical improvement in his lower extremity deficits. The efferent-afferent coupling theory worked in this case with the mental move. The mentamove® supported the patient in the early phase of the disease. It gave up support on every muscle level. It worked on the left peroneal muscles but the recovery there was slow than on the right side. We explained it with the injured fibers of the Cauda Equina. These may control the left peroneal muscles.
The mental move produced for the rehabilitation of stroke patients and CNS pathologies. Our clinical experiences showed it may be useful and work for some incomplete peripheric nerve injured patients.
These data demonstrate that Mentamove® can be successfully used to treat CES deficits after decompressed spinal surgery, with incomplete nerve injury.
Literature
- R. Crisan, C. Garner: Effectiveness of EMG-initiated muscular stimulation in outpatients one year post-stroke Neurologie & Rehabilitation 6/2001, Hippocampus Verlag, ISSN 0947-2177, S. 228-232.
- Alfieri V (1982): Electrical treatment of spasticity. Reflex tonic activity in hemiplegie patients and selected specific electrostimulation. Scand J. Rehabil Med 14, 177-82
- Bach-y-Rita P (1981): Brain plasticity as a basis of the development of rehabilitation pro-cedures for hemiplegia. Scand J Rehab Med 13, 73-83
Abstract ID: A0157
The Mentamove Rehabilitation After Traumatic Cauda Equina Syndrome (Case Report)
Dr. Christoph Garner1, Dr. Mustafa Akgün2, Dr. Zehra Akgün3
1KWA Stift Rottal Clinic Neurology and Neurorehabilitation MD, Germany, 2 State Hospital of Bursa Neurosurgery MD, Turkey, 3 Uludag University School of Health PhD, Turkey
Background: Brain Efficiency Training (Mentamove) is a neurorehabilitation method used for rehabilitation after various brain lesions. If the motoric activities are mentally practiced by the patient, the real movement gives a reorganization to the brain, due to neuroplasticity. The Mentamove Method has never been documented for use to treat Cauda Equina Syndrome (CES) deficits and paraplegia before this Case Report.
Methods: The subject of this case (a 30-year-old male) was operated on for an L2 compression fracture, 3 days after sustaining the injuries in a traffic accident. The spinal surgery used was a complete laminectomy of L2 and L3, and then the Cauda Equina was decompressed. The dura was ruptured approximately 4-5 cm and some caudal fibers were disrupted. After dural repair, the posterior spinal instrumentation was implemented. The subject had total paraplegia before and after surgery, and anesthesia was below the L1 segment. The anal tonus was lost and priapism was noted. After 5 days of the surgical decompression, the Mentamove treatment program was implemented. Mentamove was applied to the hip flexors, knee extensors, peroneal group muscles, gluteal muscles, and the hamstring muscle groups 2 times/daily bilaterally. The data was measured with the Medical Research Council Scale (MRC) 0-5 for 10 days.
Results: After 10 days, the subject was able to slightly move the toes on his right foot. Based on the MRC scale, after 30 days, he started to move the right leg from 0 to 4. And his left hip demonstrated 2-point muscle activity, and his left foot showed 2-point motor activity. After 50 days of therapy, he started to stand with assistance. After 4 months of therapy, he walked with the 5-point muscle control of the legs. He was able to control urinary incontinence and anal tonus.
Conclusion: These data demonstrate that Mentamove can be successfully used to treat CES deficits after decompressed spinal surgery, with incomplete nerve injury.
Kaynaklar ve Benzer Vakalar
- https://drmustafaakgun.com/mentamove-ile-rehabilitasyon/
- https://drmustafaakgun.com/the-mentamove-rehabilitation-2/
- https://drmustafaakgun.com/akut-spinal-kord-kompresyonu-sonrasi-paraplejide-mentamove-tedavisinin-etkisi-olgu-sunumu/
- https://drmustafaakgun.com/paraparezi-ve-mentamove/
- https://drmustafaakgun.com/bilateral-distal-paraplejide-mentamove/
- https://drmustafaakgun.com/kafa-travmasi-sonrasi-mentamove/
- https://drmustafaakgun.com/beyin-etkin-calisma-egitimi/
- https://drmustafaakgun.com/mentamove-metodu-ile-rsd-refleks-sempatik-distrofinin-tedavisi/
- https://drmustafaakgun.com/foot-drop-mentamove-metodu/
- https://drmustafaakgun.com/the-mentamove-rehabilitation/
- https://drmustafaakgun.com/the-oculomotor-palsy-after-right-posterior-communicant-aneurysm-surgery-and-treatment-with-mentamove-case-report/
- https://drmustafaakgun.com/mentamove-rehabilitasyon-nedir/
- https://drmustafaakgun.com/category/norolojik-rehabilitasyon/
- https://drmustafaakgun.com/mentamove-tedavisi/