
Dikkat: Sitemizde yayınlanan bazı bilgiler dış kaynaklardan alınmıştır. Bu kaynaklara doğrudan link verilmektedir. Pasaj sonundaki literatür bilgileri dışında başka sitelere çıkış yapma olasılığınız vardır. Tekrar geri dönmek için ilgili siteye gitmek istediğinizde yeni sekme açarak gitmeniz daha uygun olur. Doğrudan dış sitelere gittiğinizde geri dönmek isterseniz adres çubuğundan geri tuşu ile tekrar bu metne dönebilirsiniz.
Aynı şekilde başka sitelerde yayınlanmış görsellere de ulaşmak için kaynağına gidebilirsiniz. İlgili görseli kaynağında ziyaret edebilirsiniz.
Sitemizde bize ait görüntüler herhangi bir telif hakkı talep edilmeksizin kopya edilebilir, kullanılabilir. Kaynağın bizim sitemiz olduğunu belirtmeniz yeterlidir.
Sitemiz bilgilendirme amaçlıdır. Sitemize herhangi bir reklam uygulaması alınmamaktadır. Sitemiz bilgi paylaşım amaçlı olup, tıp ile ilgilenen herkese açıktır. Üyelik zorunlu değildir.
Hazırlanan içeriklerimiz tamamen amatör ruhla hazırlanmakta olup, aynı şekilde video kanalımız linki.
https://www.youtube.com/channel/UC3JBKVVaVfhI1z_rKMDUuZg/
Video kanalımız üzerinden bizi takip edebilir, abone olabilir, bize mesaj bırakabilirsiniz. Yorum bırakmanız halinde hatalarımızı düzeltmek için güncel olmamıza katkı sağlayabilirsiniz.
Tüm takipçilerimize teşekkür ederiz.
Bell Paralizisinde Mentamove Tedavisi. Bell Paralizisi olan hastamızda, 30 günlük Mentamove uygulamasından sonra yüzün sol tarafı tamamen iyileşme göstermiştir. (Mentamove Treatment in Bell’s Paralysis. In our patient with Bell’s palsy, the left side of the face completely healed after 30 days of Mentamove application)
Last Revision: 02.12.2022
Keywords: Bell Palsy, Peripheric Facial Paralysis, Electromyography, Rehabilitation, Biofeedback, Electrotherapy, Neuroplasticity, Relearning, Brain Efficiency Training, Mentamove®, Herpes Simplex
Background
The onset of paralysis is sudden with Bells palsy and Ramsey Hunt syndrome, although symptoms can worsen during the early days. Bell’s palsy symptoms typically peak within a few days, although it can take as long as 2 weeks. Ramsey Hunt syndrome symptoms will peak within 3 weeks. If paralysis develops slowly, tests for other causes of the palsy must be done. (Fig. 1)
Psychologically, facial paralysis can be devastating, particularly in cases that extend for a long period, or where residuals are significant. Friends, family, and doctors often have no true concept of how deeply the patient’s sense of self and self-esteem is affected. You will also find that they have little or no understanding of your physical discomfort, difficulty, and frustration as you struggle to do seemingly simple things that they take for granted. But the recent years there were many developments in understanding the causes of the facial nerve. There is diagnosed that the Herpes Simplex virus was hidden in the Geniculate Ganglion. [1] So this hidden virus in the future can also be reactivated and spread a second time along the facial nerve.[2]
There are many physical symptoms associated with facial paralysis, but the effects will differ between individuals. They can vary in accordance with the degree of nerve damage, and the location of the damage. [3]
| GENERAL SYMPOTMS | EYE RELATED SYMPOTMS |
| Muscle weakness or paralysis Forehead wrinkles disappear Overall droopy appearance Impossible or difficult to blink Nose runs Nose is constantly stuffed Difficulty speaking Difficulty eating and drinking Sensitivity to sound (hyperacusis) Excess or reduced salivation Facial swelling Diminished or distorted taste Pain in or near the ear Drooling | Eye closure difficult or impossible Lack of tears Excessive tearing Brow droop Tears fail to coat cornea Lower eyelid droop Sensitivity to light |
| RESIDUAL EFFECTS | ADDITIONAL SYMPTOMS WITH RAMSEY HUNT SYNDROME |
| Eye appears smaller Blink remains incomplete or infrequent Tearing abnormalities Asymmetrical smile Mouth pulls up and outward Sinus problems Nose runs during physical exertion Post paralytic hemifacial spasm Hypertonic muscles Co-contracting muscles Synkinesis (oral/ocular well known, but can affect any muscle group) Sweating while eating or during physical exertion Muscles become more flaccid when tired, or during minor illness Muscles stiffen when exposed to cold, when tired, or during illness | Hearing deficit Severe pain Long lasting pain Vertigo Blisters in ear or other areas Nausea |
Although the damage that causes the paralysis is specific to the 7th nerve, other nerves may be temporarily irritated. For example, temporary facial numbness or pain can result when CN-V is irritated. [4]
Recovery is not consistent among patients. For some people the mouth may move before the ability to blink returns; in others it will be eyelids first and mouth last. Twitching may precede movement, but it doesn’t always. Pain in areas starting to “wake up” may occur, or may not. The sense of taste can be odd as the sensation returns, or the sense of taste may return without any awareness of the change. Recovery can be gradual, rapid, or hit occassional plateaus. [4]
RESIDUAL EFFECTS
Residuals may be due to one, or a combination of several factors. Initial trauma to the nerve can be minor and temporary, or significant and long-lasting. When the damage is minor, recovery is likely to be essentially complete, and rapid. With more extensive damage, other factors begin to affect recovery. [4]
In longer recoveries, other cranial nerves may try to take over for the 7th nerve, growing into passageways formerly occupied by the 7th nerve. Also, the 7th nerve can regenerate incorrectly, taking some different paths than it had followed before Bell’s palsy. The result is “crossed wiring” and synkinesis, which are further described in the next section. [4]
After paralysis, facial muscles tend to become hypertonic. This means they tend to be overactive, contracting when they should be at rest. Typical signs are a squinty eye, the mouth pulled up, a sore or swollen cheek, and deepened creases. Unlike skeletal muscles, facial muscles lack spindles. Muscle spindles sense when a muscle is in a contracted state, and nerves can send the appropriate signal to the muscle telling it to relax. Without these spindles, there is no awareness of the contraction, and the muscles remain in a state of tension. A muscle that can not fully relax also can not fully contract, so the range of motion becomes limited. [4]
Learned misuse and disuse of the muscles also can affect both appearance and mobility. While the muscles are paralyzed, it’s natural to try to eat, drink and speak, etc., as well as you can. New habits may be learned while you’re compensating for the nonworking muscles. You may inadvertently call on inappropriate muscles to join forces and work together to accomplish movements that aren’t happening on their own (learned misuse). Or you may become accustomed to compensating without using the lazy muscles (learned disuse). The effects of both may remain after nerve function returns. Both can also affect the “good” side, which may have learned unnatural patterns while its muscles were assisting the nonworking muscles. [4]
Physical therapy can minimize the asymmetrical appearance and improve mobility, even when therapy is started years after the initial paralysis. [4]
Brain Efficiency Training (Mentamove®) is a neurorehabilitation method used for rehabilitation after brain lesions. If the motoric activities are mentally practiced by the case, the real movement gives a reorganization to the brain. EMG-initiated muscular stimulation gives is an effect mainly used in the treatment of stroke patients. It is a combination of muscular stimulation with medium-frequency sine current and a biofeedback process (5,6).
We presented a case treating on bilateral traumatic facial nerve lesions with Mentamove® at the 4 WCNR 2006 in Hong Kong (7).
Our opinion comes from the biofeedback coupling theory and if the method works truly it may be given a positive effect on the central nervous system for recovery (Fig 2).
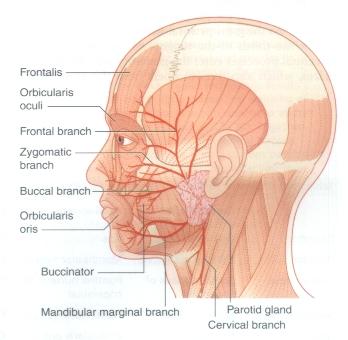
The efferent and afferent ways of the peripheric nervous system work with different peripheric nerves. The motor fibers (efferent) of the facial nerve come from the facial nuclei of the brain stem. These nuclei are under the mental motor control of the temporal lobe bilaterally. But the sensorial ways (afferent) work with the trigeminal nerve and brain stem. (8)
Our treatment theory to work with mentamove® bases on incomplete motor facial nerve fibers injury and healthy trigeminal nerve fibers. So we are believing to treat the Bell Palsy Case with Mentamove® in this report. And before therapy, we would like to presentate the beginning treatment protocol of the therapy and have to get show the survival of this case to the other Mentamove® appliers and therapists.
 |
Fig 2: EMG controlled back coupling is a real time working system for paretic subjects
Case
This case is 66 years old woman. She had a left facial paralysis (Bell Palsy) 10 days ago (Fig. 3, 4, 5, 6). The Cranial MRI shows normal brain signs and brain stem structure. There is no pontocerebellar angle pathology (like tumor and vascular pathology). The subject says only she has a big psychologic stress due to die her husband. There is no trauma or infection like HSV before the facial paralysis. She doesn’t have diabetes or any malignancies. Only she shows chronic bronchitis. Clinically she shows left-side facial paralysis, with an inability to close the eyelid.
 |
Fig. 3, 4, 5, 6: Before of the mentamove treatment left side peripheric type of facial paralysis. These pictures were taken before the therapy. (Bell Paralizisinde Mentamove Tedavisi)
 |
Fig. 7, 8, 9, 10: After 15 days of the mentamove therapy these pictures have been showing here.
 |
Fig. 11, 12, 13, 14: After 30 days of the mentamove therapy shows symmetrical improvement of the left facial paralysis. And the ability to close the eyelid.
Method
After 10 days of facial paralysis, the mentamove® therapy was implemented. The Mentamove® treatment protocol was given on the left facial mimic muscles (m.orbicularis oris). She concentrates to smile on the front of the mirror, because she is a very very beautiful woman, then triggers the mentamove® to stimulate facial muscles. The courses took 20 minutes per day.
Results
There are no changes on the left side facial muscles during the 10 days before implementation of the mentamove® treatment. During the first course of the mentamove®, she showed only a little contraction during electrostimulation and she can trigger the electrostimulation with a 5 mV offset value. The intensity was applied at 7 mAmp.The therapy was completed after 30 courses. There was no any complication during therapy.
Conclusion
We have the background to treat these cases with mentamove® and our experimental workings showed a good recovery after treatment.
In this case, we would like to presentate and show how the treatment survives continually.
During the first 15 days, the patient showed about 50 % improvement in the left side asymmetry.
After 30 days of application, the patient showed total recovery on the left face. She can do contractions on the facial muscle voluntarily. She can smile symmetrically after treatment.
The standard rehabilitation techniques (TENS, massages on the face, muscle stimulations, acupuncture) may be used in the treatment of facial paralysis. These techniques don’t consist of mental training.
The peripheral muscle stimulation doesn’t give any mental control activity on the muscle.
While the Mentamove® treatment method is used for these patients they try to contract muscles on their faces. When the subject tries to smile in front of the mirror the mental imagery this activity gives increasing EMG signals in the facial muscles, during these EMG signals increasing in the facial muscles and electrostimulation begins. This application gives a real muscle contraction, on the subject which takes power from muscle stimulation and contractions, and it completes biofeedback effects from muscle. This method can be used regularly on peripheral facial palsies.
Refferences
- https://pubmed.ncbi.nlm.nih.gov/15699730/
- https://pubmed.ncbi.nlm.nih.gov/9393551/
- https://my.clevelandclinic.org/health/diseases/5457-bells-palsy
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2848459/
- R. Crisan, C. Garner: Effectiveness of EMG-initiated muscular stimulation in outpatients one year post-stroke Neurologie & Rehabilitation 6/2001, Hippocampus Verlag, ISSN 0947-2177, S. 228-232.
- Adams JA (1971): A closed-loop theory of motor learning. J. Motor Behav 3, 111-49
- The Mentamove Rehabilitation after Bilateral Facial Paralysis and Brachial Plexus Injury (Case Report): Z. Akgun1, M. Akgun2, C. Garner3. 1 Uludag University School of Health PhD, TURKEY, 2 State Hospital of Bursa Neurosurgery MD, TURKEY, 3 KWA Stift Rottal Clinic Neurology and Neurorehabilitation MD, GERMANY . Nurorehabilitation&Neural Repair, Vol: 20, Number 1, March 2006, p:190.
- https://www.ncbi.nlm.nih.gov/books/NBK554569/